Fractyl Health Reports Positive Randomized Data from REMAIN-1 Midpoint Cohort Demonstrating Durable Weight Maintenance One Year After GLP-1 Discontinuation
Rhea-AI Summary
Fractyl Health (Nasdaq:GUTS) reported one-year randomized data from the REMAIN-1 Midpoint Cohort evaluating the Revita DMR System for post-GLP-1 weight maintenance after tirzepatide discontinuation. In the mITT population (N=45), least-squares mean weight regain was 7.8% with Revita versus 13.0% with sham at one year.
Among participants with complete duodenal ablation (>14 cm), Revita patients maintained about 81% of GLP-1-induced weight loss versus 48% with sham, corresponding to 4.8% versus 13.0% weight regain. In an optimized subgroup (complete ablation and ≥17.5% run-in weight loss), approximately 84% of weight loss was maintained with Revita versus 46% with sham (4.1% versus 13.5% regain).
The weight-maintenance responder rate reference for the Pivotal Cohort was 73% in the Midpoint mITT population and 91% with complete ablation. No device- or procedure-related serious adverse events were reported, TEAE rates were similar between arms, and no new device-related TEAEs occurred from six to 12 months. Fractyl highlighted upcoming milestones: topline six-month Pivotal Cohort data in early Q4 2026 and a potential FDA De Novo submission in late Q4 2026.
Positive
- Weight regain reduced ~40% at one year versus sham in mITT (7.8% vs 13.0%)
- Complete ablation subgroup retained ~81% of GLP-1 weight loss vs 48% with sham
- Optimized subgroup retained ~84% of GLP-1 weight loss vs 46% with sham
- Responder rate reference 73% in mITT, 91% with complete duodenal ablation
- No device- or procedure-related serious adverse events reported through one year
- TEAE rates comparable between Revita and sham (24% vs 25%) at one year
Negative
- Midpoint Cohort subgroup described as exploratory and not powered for formal inference
- Pivotal Cohort primary endpoint still pending; only reference responder data available
- Sample sizes limited in key subgroups (e.g., optimized subgroup Revita n=10, sham n=8)
News Market Reaction – GUTS
On the day this news was published, GUTS gained 13.75%, reflecting a significant positive market reaction. Argus tracked a peak move of +20.0% during that session. Argus tracked a trough of -7.3% from its starting point during tracking. Our momentum scanner triggered 28 alerts that day, indicating elevated trading interest and price volatility. This price movement added approximately $20M to the company's valuation, bringing the market cap to $161.82M at that time. Trading volume was exceptionally heavy at 5.7x the daily average, suggesting very strong buying interest.
Data tracked by StockTitan Argus on the day of publication.
Key Figures
Historical Context
| Date | Event | Sentiment | 24h Move | Catalyst |
|---|---|---|---|---|
| Jun 04 | Clinical data update | Positive | -3.5% | Reported positive one-year open-label REVEAL-1 Revita weight-maintenance data. |
| Jun 01 | Leadership appointment | Positive | +7.6% | Hired SVP for market access and commercial strategy ahead of key Revita milestones. |
| May 12 | 1Q26 earnings report | Positive | +29.2% | Posted net income, detailed cash runway into early 2027, and trial progress. |
| May 11 | Clinical trial authorization | Positive | +1.9% | Received authorization to begin first-in-human trial of RJVA-001 in T2D. |
| May 05 | Earnings date notice | Positive | -4.6% | Announced date for Q1 2026 results and participation in investor conference. |
24h Move is the share-price change in the day after each event; other market factors may also have contributed.
The stock has often risen on positive clinical and financial updates, though there are instances where favorable news coincided with short-term declines.
Key Terms
modified intention-to-treat medical
least-squares mean medical
mixed-model repeated measures medical
treatment-emergent adverse events medical
de novo marketing application regulatory
AI-generated analysis. How Rhea-AI works. Not financial advice.
Up to
Next anticipated Revita® milestones are topline six-month randomized data from the REMAIN-1 Pivotal Cohort in early Q4 2026 and a potential FDA De Novo marketing application submission in late Q4 2026
Company to host investor webcast today at 8:00 a.m. ET
BURLINGTON, Mass., July 15, 2026 (GLOBE NEWSWIRE) -- Fractyl Health, Inc. (Nasdaq: GUTS) (the Company or Fractyl), a clinical-stage metabolic therapeutics company focused on pioneering novel approaches to treat obesity and type 2 diabetes (T2D), today announced positive one-year results from its REMAIN-1 Midpoint Cohort (“Midpoint Cohort”). The new results reinforce the potential of the Revita DMR System (Revita) to be the first durable procedural therapy for post-GLP-1 weight maintenance.
Key Findings:
- Dose-dependent durability confirmed at one year: In the full modified intention-to-treat (mITT) population (N=45), a single Revita procedure reduced weight regain by approximately
40% versus sham at one year (least-squares mean weight regain of7.8% versus13.0% of body weight; n=29 versus 16 for Revita versus sham). Participants who received complete duodenal ablation (>14 cm) maintained approximately81% of GLP-1-induced weight loss at one year, compared with48% in sham participants (least-squares mean weight regain of4.8% versus13.0% of body weight; n=17 versus 16 for Revita versus sham), reflecting a reduction in weight regain of over60% versus sham. This is consistent with earlier findings that more complete duodenal ablation drives greater treatment effect.
- Greatest benefit in patients with greatest need: In an optimized population of participants who received complete duodenal ablation (>14 cm) and had higher GLP-1 run-in weight loss (≥
17.5% ), Revita maintained approximately84% of GLP-1-induced weight loss at one year versus46% with sham (least-squares mean weight regain of4.1% versus13.5% of body weight; n=10 versus 8 for Revita versus sham). These results are consistent with the view that patients at greatest need may derive the greatest benefit from Revita due to their higher propensity for weight regain after GLP-1 discontinuation.
- Weight-maintenance responder rate: The second co-primary endpoint of the Pivotal Cohort, assessed against a U.S. Food and Drug Administration (FDA) mandated pre-specified performance goal of >
50% , measures the proportion of Revita patients maintaining at least5% total body weight loss relative to their pre-tirzepatide weight at one year. As a reference point for the Pivotal Cohort, this responder rate was73% in the Midpoint Cohort mITT population, rising to91% in those with complete duodenal ablation (>14 cm).
- Excellent tolerability: No device- or procedure-related serious adverse events occurred. No new device-related treatment-emergent adverse events (TEAEs) were observed between six and 12 months. Overall TEAE rates were comparable between arms through one year (
24% Revita versus25% sham), reflecting a generally mild peri-procedural adverse event profile that supports potentially broad outpatient use for Revita. One new diagnosis of type 2 diabetes occurred in the sham arm versus none with Revita.
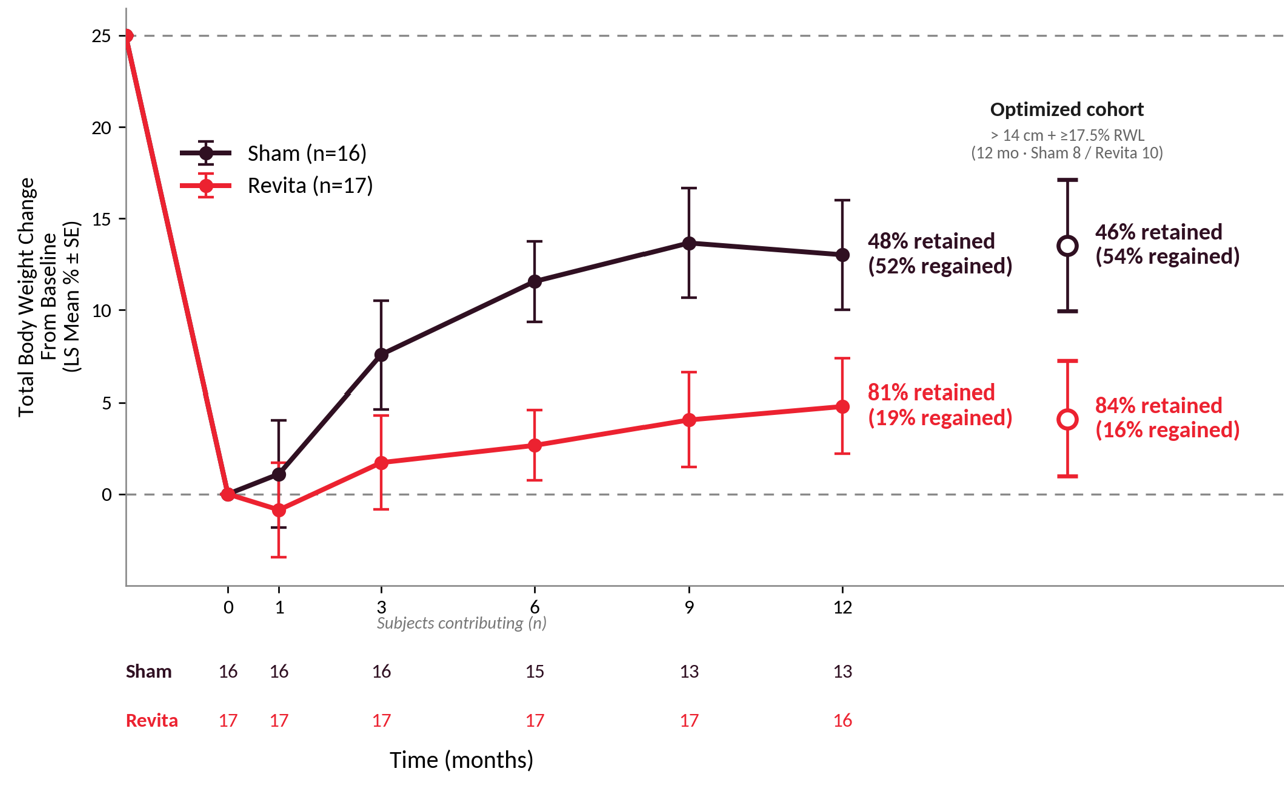
Figure 1: Change in body weight in (i) Complete Ablation population: > 14 cm duodenal ablation, no run-in weight loss restriction (Sham n=16, Revita n=17) and (ii) Optimized population: complete ablation (> 14 cm) and run-in weight loss ≥
“The success of GLP-1 medicines has created a new unsolved problem: what happens when patients stop. Most do stop eventually, whether because of cost, side effects, or simply not wanting to inject a drug for the rest of their lives. When they stop, the weight most often comes back,” said Harith Rajagopalan, M.D., Ph.D., Co-Founder and Chief Executive Officer of Fractyl. “Today's results are the first randomized, sham-controlled evidence that a single Revita procedure can keep most of the weight off for a full year after GLP-1 is stopped, without the need for ongoing medication. We eagerly anticipate an early Q4 2026 topline readout from the REMAIN-1 Pivotal Cohort with deep conviction that Revita may represent the first procedural entrant into the post-GLP-1 weight maintenance category.”
Webcast
Fractyl Health will host a webcast today, July 15, 2026, at 8:00 a.m. Eastern Time. The live webcast can be accessed by clicking this link. This webcast can also be found in the “Events” section of Fractyl’s website at ir.fractyl.com. The webcast will be archived and available for replay for at least 30 days after the event.
About REMAIN-1 Weight Maintenance Program
REMAIN-1 is Fractyl Health’s pivotal program evaluating Revita for weight maintenance in adults with obesity following discontinuation of GLP-1 therapy. The Midpoint Cohort (N=45) is a randomized, double-blind, sham-controlled study in adults who achieved at least
About Revita
Revita is Fractyl Health’s lead product candidate, designed to remodel the duodenal lining via a one-time, minimally invasive endoscopic procedure intended to restore healthy nutrient sensing and signaling disrupted by chronic metabolic disease. Revita has received Breakthrough Device designation from the FDA for weight maintenance in people with obesity who discontinue GLP-1 therapies. Revita is for investigational use only in the United States and is CE marked in the European Union and United Kingdom.
About Fractyl Health
Fractyl Health is a clinical-stage metabolic therapeutics company advancing two differentiated candidates designed to target the root causes of obesity and T2D: Revita, a procedural therapy in pivotal development for post-GLP-1 weight maintenance, and Rejuva, an AAV-based gene therapy platform with its lead candidate RJVA-001 entering first-in-human clinical studies. Fractyl’s goal is to advance metabolic disease treatment from chronic management toward prevention and reversal of disease. Fractyl is headquartered in Burlington, Massachusetts.
Forward-Looking Statements
This press release contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. All statements contained in this press release that do not relate to matters of historical fact are forward-looking statements. These statements may be identified by words such as “aims,” “anticipates,” “believes,” “could,” “estimates,” “expects,” “forecasts,” “goal,” “intends,” “may,” “plans,” “possible,” “potential,” “seeks,” “will” and variations of these words or similar expressions that are intended to identify forward-looking statements, although not all forward-looking statements contain these words. Forward-looking statements in this press release include, without limitation, statements regarding: the promise and potential impact of our clinical trial data and product candidates, including Revita’s potential for maintaining weight loss after GLP-1 based therapy discontinuation and stabilizing cardiometabolic parameters; the translatability of results and scalability of technique related to Revita; the design, initiation, timing and results of clinical enrollment and any clinical studies or readouts, including readouts from the REMAIN-1 Midpoint Cohort and the REMAIN-1 Pivotal Cohort; the potential launch or commercialization of any of our product candidates or products; our regulatory strategy, including potential use and benefits of the De Novo pathway (FDA pre-submission feedback is advisory and non-binding, and there is no assurance that FDA will accept a De Novo marketing application submission or that Revita will receive marketing authorization); the potential treatment population or benefits for any of our product candidates or products; our strategic and product development objectives and goals; and the timing of any of the foregoing. These statements are neither promises nor guarantees, but involve known and unknown risks, uncertainties and other important factors that may cause our actual results, performance or achievements to be materially different from any future results, performance or achievements expressed or implied by the forward-looking statements, including, but not limited to, the risks that are discussed more fully in our filings with the Securities and Exchange Commission (the SEC), including the “Risk Factors” section of our Annual Report on Form 10-K for the year ended December 31, 2025, filed with the SEC on March 24, 2026, and other documents we subsequently file with or furnish to the SEC, including our Quarterly Report on Form 10-Q for the quarter ended March 31, 2026, filed with the SEC on May 12, 2026. These forward-looking statements are based on management’s current estimates and expectations. While we may elect to update such forward-looking statements at some point in the future, we disclaim any obligation to do so, even if subsequent events cause our views to change.
Contact
Brian Luque, Head of Investor Relations and Corporate Development
IR@fractyl.com, 951.206.1200
A photo accompanying this announcement is available at https://www.globenewswire.com/NewsRoom/AttachmentNg/7554f2be-93cb-47c9-97a3-76e4a063f6c5
